Can assisted reproductive technologies like PIEZO-ICSI improve your IVF success? Yes, this technology is being employed by advanced IVF clinics to help increase fertilization rates of your eggs, thus resulting in higher numbers of better-quality embryos, giving you higher chances of success with each cycle.
Let’s explore what it is, how it works, and why it’s making waves in the world of fertility treatments.
What Is PIEZO-ICSI?
PIEZO is Greek for ‘pressure’ or ‘push.’ PIEZO-ICSI stands for Piezo-activated intracytoplasmic sperm injection. It is an advanced technique used to fertilize eggs.
In traditional ICSI, a sharp needle injects sperm into the egg by piercing its outer membrane. This method can sometimes damage delicate eggs, particularly in older women with fragile eggs.
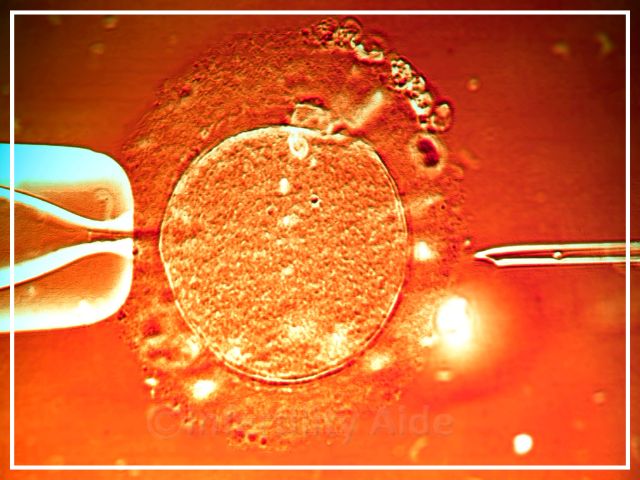
On the other hand, PIEZO-ICSI, uses a blunt needle combined with micro-vibrating motions—a gentler approach that reduces the risk of any damage to the eggs.
“We use a special injection technique for the sperm, meaning we inject the sperm into the eggs, it’s called PEIZO-ICSI,” said Dr. Leong, one of our top doctors for IVF in Malaysia. “It’s mechanical instead of purely manual,” so the chances of human error are reduced.
How does PIEZO-ICSI help?
PIEZO-ICSI offers several advantages over conventional methods:
- Improved fertilization rates
A cohort study found fertilization rates of 80.5% with PIEZO-ICSI, compared to 65.8% with traditional ICSI. - Minimized egg damage
The gentler, mechanical action reduces the risk of damaging fragile eggs, especially in women with advanced age or lower egg quality. The study cited above found oocyte degeneration rates to be only 4.4% with PIEZO ICSI vs 8.6% in conventional ICSI. - Better embryo quality
By preserving the egg’s integrity, PIEZO-ICSI can lead to embryos of higher quality, boosting the chances of implantation. - Ideal for older women
Women aged 38+ or those with poor fertilization rates from previous IVF cycles may benefit most.
Is IVF more successful with ICSI?
ICSI has revolutionized IVF, particularly for couples facing male-factor infertility. PIEZO-ICSI takes this a step further by refining the injection process.
A higher fertilization rate often means more embryos to work with, increasing the likelihood of success in IVF across fresh or frozen embryo transfer cycles.

How much does PIEZO-ICSI cost?
The clinics that do employ PEIZO-ICSI, do not normally charge extra for the technology but their services might be slightly more expensive overall, than those that don’t.
You do not want to save small amounts of money and go for cheaper technology, only to risk an entire IVF cycle. Ask your clinic about these technologies, so you can take advantage of the best that science has to offer today and give yourself the highest chances of success in IVF.
Is there any downside to ICSI?
While ICSI, including PIEZO-ICSI, is highly effective, there are some considerations:
- Cost – Advanced methods like PIEZO-ICSI can add to the overall cost of IVF.
- Egg handling risks – Though highly effective, ICSI carries a small risk that is much lower in PIEZO-ICSI.
- Availability – PIEZO-ICSI is not yet widely available. You may need to find a specialized clinic to be able to use this technology.
Where can I get PIEZO-ICSI?
This service is available with some of our IVF doctors in Thailand, Malaysia, and Mexico.
Innovations like PIEZO-ICSI can help improve your IVF success by reducing the risks to fragile eggs and improving the egg fertilization rate.
If you’re considering IVF, and wish to consult with an experienced fertility expert about PIEZO-ICSI, find your IVF clinic here.
References
Kelton Tremellen, PIEZO-ICSI increases fertilization rates compared with standard ICSI: a prospective cohort study, Reproductive BioMedicine Online, ISSN 1472-6483. DOI: https://doi.org/10.1016/j.rbmo.2021.05.020.
Caddy, M., Popkiss, S., Weston, G., Vollenhoven, B., Rombauts, L., Green, M., & Zander-Fox, D. (2023). PIEZO-ICSI increases fertilization rates compared with conventional ICSI in patients with poor prognosis. Journal of assisted reproduction and genetics, 40(2), 389–398. https://doi.org/10.1007/s10815-022-02701-y
Reviewd by: Dr. Meenakshi, PhD